
From April 1st, 2013, to March 31st, 2014, 44 hemodialysis units took part in the surveillance of vascular access–related bloodstream infections (VARBSIs) in hemodialysis (HD) patients, for a combined total of 54,878 patient-periods (Table 1). Participating units reported 157 VARBSIs in 149 patients. Patient-periods involving a fistula accounted for 44.9% of patient-periods. The VARBSI incidence rate was 0.10 cases per 100 patient-periods for patients with an arteriovenous (AV) fistula, 0.22 for patients with a synthetic fistula (graft), 0.38 for patients with a permanent catheter and 6.20 for patients with a temporary catheter. In 2013-2014, incidence rates were stable for patients with a graft and for patients with a temporary catheter compared to 2009-2013, while incidence rates decreased significantly for patients with an AV fistula as well as patients with a permanent catheter. In 2013-2014, three HD units opened up and joined the program; one HD unit carried out the surveillance but could not report its results so these were excluded from analysis. Data was extracted on May 15, 2014.
Update: March 9, 2017
Table 1 – Participation of Hemodialysis Units in the Surveillance of VARBSIs in Hemodialysis Patients, Québec, 2009-2010 to 2013-2014
2009-2010 | 2010-2011 | 2011-2012 | 2012-2013 | 2013-2014 | |
|---|---|---|---|---|---|
| Units (N) | 26 | 30 | 42 | 42 | 44 |
| Patients monitored (average number per period) | 3,035 | 3,337 | 3,871 | 3,977 | 4,221 |
| Patient-periods* (N) | 39,458 | 43,387 | 50,327 | 51,697 | 54,878 |
| Patient-months (N) | 36,947 | 40,607 | 47,245 | 48,340 | 51,362 |
| Dialysis sessions (N) | 475,033 | 522,087 | 607,436 | 621,516 | 660,365 |
| Catheter-days (N) | 592,317 | 659,463 | 753,432 | 798,816 | 847,947 |
| VARBSIs (cat. 1a, 1b and 1c, N) | 199 | 191 | 216 | 218 | 157 |
| VARBSIs with AV fistulas or grafts (N) | 35 | 30 | 38 | 46 | 27 |
| VARBSIs with permanent or temporary catheters (N) | 164 | 161 | 178 | 172 | 130 |
| Infected patients (N) | 186 | 182 | 208 | 209 | 149 |
* A period corresponds to 28 days for a total of 13 periods per year.
Incidence Rates
In 2013-2014, the VARBSI incidence rate was 0.10 cases per 100 patient-periods for patients with an AV fistula, 0.22 for patients with a graft, 0.38 for patients with a permanent catheter and 6.20 for patients with a temporary catheter (Figure 1). The VARBSI incidence rate was higher when the buttonhole technique was used (0.25 per 100 patient-periods versus 0.02, p < 0.01). Incidence rates were not statistically different between patients with permanent catheter, graft nor AV fistula with buttonhole.
Therefore, compared with an AV fistula without buttonhole, the incidence rate with a temporary catheter was 305.0 [88.9 ; 1046.6] times greater, with a permanent catheter, 18.5 [6.0 ; 58.9] times greater, with a graft 10.7 [2.6 ; 44.8] times greater and with an AV fistula with a buttonhole, the incidence rate was 12.3 [3.6 ; 41.5] times greater (all p values < 0.01). The incidence rate with a temporary catheter was 16.3 [9.7 ; 27.5] times higher than with a permanent catheter (< 0.01).
Figure 1 – VARBSI Incidence Rate by Type of Vascular Access, Québec, 2013-2014 (Incidence Rate per 100 Patient-periods [95% CI])
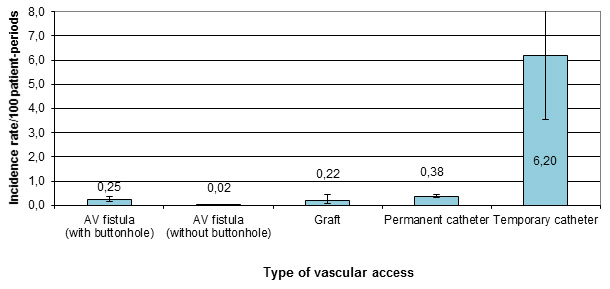
95% CI: 95% confidence interval
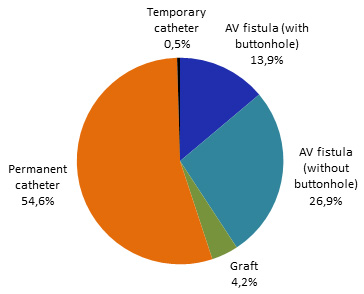
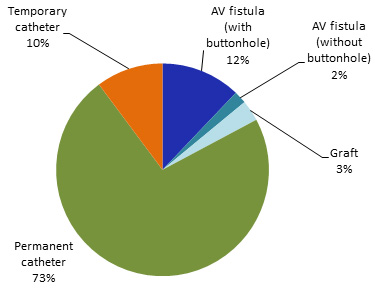
Permanent catheters are the most commonly used type of vascular access, followed by AV fistulas without the use of the buttonhole technique (Figure 2).
Figure 2 – Breakdown of Patient-periods by Type of Vascular Access, Québec, 2013-2014 (%)
Incidence Rate Time Trends
In 2013-2014, the incidence rates for patients with a graft and patients with a temporary catheter were comparable to 2009-2013 rates (Table 2 and Figures 3 and 4). However, the incidence rate for patients with AV fistula decreased significantly (p < 0.01) just as for patients with permanent catheter (p < 0.01). This decrease, observed with the two most frequently used types of vascular access, must be viewed in parallel with the sharp drop of VARBSI cases reported in 2013-2014 (Tables 2 and 3).
Figure 3 – VARBSI Incidence Rates by Type of Vascular Access, Québec, 2009-2013 and 2013-2014 (Incidence Rate per 100 Patient-periods [95% CI])
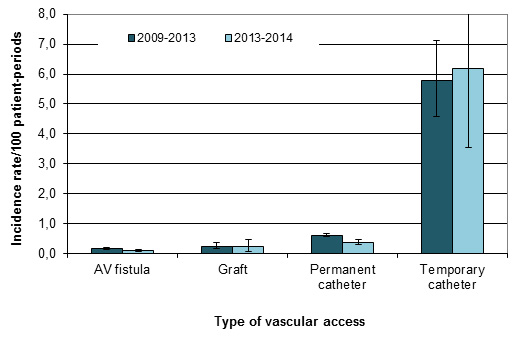
Table 2 – VARBSI Incidence Rates by Type of Vascular Access, Québec, 2009-2013 and 2013-2014 (Incidence Rate per 100 Patient-periods and per 1,000 Vascular-Access Days [95% CI])
| Type of Vascular Access | Incidence Rate/100 Patient-periods | Incidence Rate/1,000 Vascular-Access Days | ||
|---|---|---|---|---|
2009-2013 | 2013-2014 | 2009-2013 | 2013-2014 | |
| AV fistula or graft | 0.18 [0.15 ; 0.20] | 0.11 [0.07 ; 0.16] | --- | --- |
| AV fistula | 0.17 [0.14 ; 0.20] | 0.10 [0.06 ; 0.14] | --- | --- |
| Graft | 0.25 [0.16 ; 0.36] | 0.22 [0.07 ; 0.45] | --- | --- |
| Permanent or temporary catheter | 0.68 [0.63 ; 0.73] | 0.43 [0.36 ; 0.51] | 0.24 [0.22 ; 0.26] | 0.15 [0.13 ; 0.18] |
| Permanent catheter | 0.61 [0.56 ; 0.65] | 0.38 [0.32 ; 0.46] | 0.22 [0.20 ; 0.23] | 0.14 [0.11 ; 0.16] |
| Temporary catheter | 5.77 [4.57 ; 7.11] | 6.20 [3.54 ; 9.61] | 2.05 [1.63 ; 2.53] | 2.19 [1.25 ; 3.40] |
| Total | 0.45 [0.42 ; 0.48] | 0.29 [0.24 ; 0.33] | 0.24 [0.22 ; 0.26] | 0.15 [0.13 ; 0.18] |
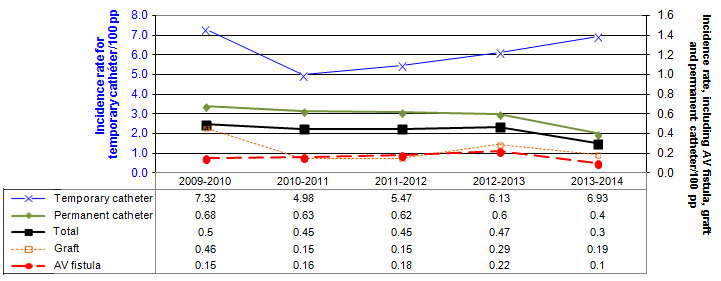
Figure 4 – VARBSI Incidence Rates by Type of Vascular Access, for Units Participating Since 2009-2010 (N = 26), Québec, 2009-2010 to 2013-2014 (Incidence Rate per 100 Patient-periods)
Despite recommendations to increase the use of fistula, the proportion of patients who receive hemodialysis through a catheter, either temporary or permanent, increased in 2013-2014 compared with 2009-2013. However, the proportion of patients with a temporary catheter, which is the form of vascular access most likely to lead to a VARBSI, decreased significantly (p < 0.01).
Table 3 – Breakdown of Patient-periods by Type of Vascular Access, 2009-2013 and 2013-2014 (%)
| Type of Vascular Access | Québec (%) | |
|---|---|---|
2009-2013 | 2013-2014 | |
| AV fistula | 41.2 | 40.8 |
| With buttonhole |
| 13.9 |
| Without buttonhole |
| 26.9 |
| Graft | 4.8 | 4.2 |
| Permanent catheter | 53.2 | 54.6 |
| Temporary catheter | 0.7 | 0.5 |
| Fistule artérioveineuse ou synthétique | 46.0 | 44.9 |
| Cathéter permanent ou temporaire | 54.0 | 55.1 |
| Catheterized for < 90 days | - | - |
| Catheterized for ≥ 90 days | - | - |
| Total (N) | 184,699 | 54,662 |
Description of cases
Patients who developed a VARBSI were aged between 0 and 93 years, with a median age of 68 years. The vast majority (83%, or 130 cases) of VARBSIs occurred in patients who received their hemodialysis treatment via catheter, even though they represented only 55% of the patient-periods monitored (Figure 5). For most of the cases that arose in patients receiving their hemodialysis through an AV fistula, the buttonhole technique was used (86%) even though this technique is used among 34% of patients with AV fistula.
Figure 5 – Breakdown of VARBSIs by Type of Vascular Access, Québec, 2013-2014 (N = 156)
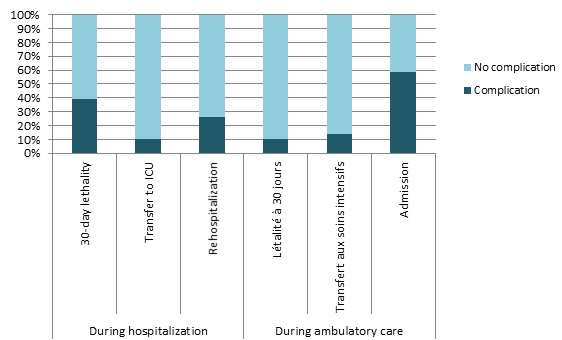
Overall, 15% of VARBSI cases resulted in death within 30 days following the onset of bacteremia. Death occurred in 39% of cases of VARBSI among hospitalized patients (Table 4 and Figure 6), compared with 11% of cases among patients receiving ambulatory care (p = 0.003). A total of 59% of ambulatory patients who developed a VARBSI required hospitalization.
Table 4 – 30-Day Case Fatality, Percentage of Transfers to ICU and Percentage of Hospitalizations and Rehospitalizations During a VARBSI Episode, by Origin of Acquisition, Québec, 2013-2014 (N, %)
| Origin of Acquisition | Complication | Number of VARBSI Cases Monitored | Presence of complication | |
|---|---|---|---|---|
N | % | |||
| During hospitalization | Death within 10 days | 23 | 5 | 22 |
| Death within 30 days | 23 | 9 | 39 | |
| Transfer to ICU | 19 | 2 | 11 | |
| Rehospitalization | 23 | 6 | 26 | |
| During ambulatory care | Death within 10 days | 134 | 9 | 7 |
| Death within 30 days | 134 | 14 | 11 | |
| Transfer to ICU | 133 | 18 | 14 | |
| Hospitalization | 134 | 79 | 59 | |
Figure 6—30-Day Case Fatality, Percentage of Transfers to ICU and Percentage of Hospitalizations and Rehospitalizations During a VARBSI Episode, by Origin of Acquisition, Québec, 2013-2014 (%)
Microbiology
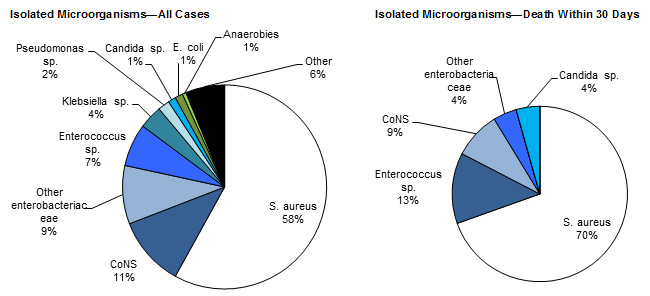
Figure 7 shows that Staphylococcus aureus was the most frequently isolated microorganism in all VARBSI cases (54%). This was followed by coagulase-negative Staphylococcus (CoNS, 11%) and Enterobacteriaceae (other than Escherichia coli and Klebsiella sp., 9%). Three of the CoNS cases (n = 18) involved S. lugdunensis. S. aureus was the most frequently isolated microorganism in cases resulting in death (70%).
Figure 7 – Categories of Isolated Microorganisms in All Reported Cases (N = 162) and Cases Resulting in Death Within 30 Days (N = 23), Québec, 2013-2014 (%)
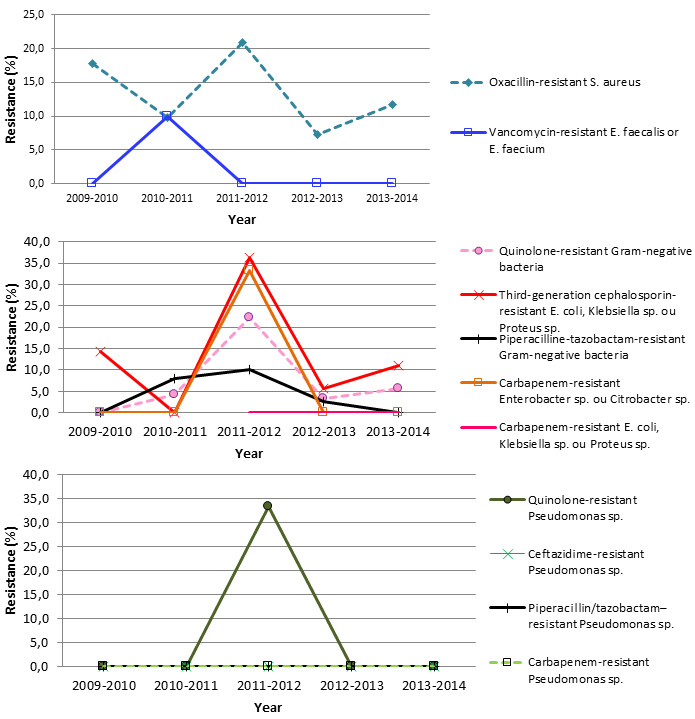
In 2013-2014, 12% of S. aureus strains were oxacillin-resistant, which is not significantly different compared with 2009‑2013 mean percentage (Table 5 and Figure 8).
Table 5 – Percentage of Strains Tested and Percentage of Resistance to Antibiotics for Certain Isolated Microorganisms, Québec, 2013-2014 (N, %)
| Microorganism | Antibioti | Isolated | Tested | Resistant | ||
|---|---|---|---|---|---|---|
N | n | % | n | % | ||
| Staphylococcus aureus | Oxacillin | 94 | 94 | 100.0 | 11 | 11.7 |
| Enterococcus faecium | Vancomycin | 2 | 2 | 100.0 | 0 | 0.0 |
| Enterococcus faecalis | Vancomycin | 7 | 7 | 100.0 | 0 | 0.0 |
| Klebsiella (pneumoniae-oxytoca) | CSE 4 | 0 | - | - | - | - |
| Imipenem or meropenem | 0 | - | - | - | - | |
| Multiresistant 1 | 0 | - | - | - | - | |
| Escherichia coli | CSE 4 | 2 | 1 | 50.0 | 1 | 100.0 |
| Fluoroquinolones 3 | 2 | 2 | 100.0 | 1 | 50.0 | |
| Imipenem or meropenem | 2 | 0 | 0.0 | 0 | - | |
| Multiresistant 1 | 2 | 1 | 50.0 | 0 | 0.0 | |
| Enterobacter sp. | CSE 4 | 3 | 3 | 100.0 | 0 | 0.0 |
| Imipenem or meropenem | 3 | 3 | 100.0 | 0 | 0.0 | |
| Multiresistant 1 | 3 | 3 | 100.0 | 0 | 0.0 | |
| Pseudomonas sp. | Amikacin, gentamicin or tobramycin | 3 | 2 | 66.7 | 0 | 0.0 |
| CSE 2 | 3 | 3 | 100.0 | 0 | 0.0 | |
| Fluoroquinolones 2 | 3 | 3 | 100.0 | 0 | 0.0 | |
| Imipenem or meropenem | 3 | 3 | 100.0 | 0 | 0.0 | |
| Piperacillin/tazobactam | 3 | 3 | 100.0 | 0 | 0.0 | |
| Multiresistant 2 | 3 | 3 | 100.0 | 0 | 0.0 | |
| Acinetobacter sp. | Imipenem or meropenem | 1 | 1 | 100.0 | 0 | 0.0 |
| Multiresistant 3 | 1 | 1 | 100.0 | 0 | 0.0 | |
CSE 2: cefepime or ceftazidime;
CSE 4: cefepime, cefotaxime, ceftazidime or ceftriaxone;
Fluoroquinolones 2: ciprofloxacin or levofloxacin;
Fluoroquinolones 3: ciprofloxacin, levofloxacin or moxifloxacin;
Multiresistant 1: intermediate or resistant to an agent in three of the following five categories: cephalosporins 4, fluoroquinolones 3, aminoglycosides, carbapenems, piperacillin or piperacillin/tazobactam.
Multiresistant 2: intermediate or resistant to an agent in three of the following five categories: cephalosporins 2, fluoroquinolones 2, aminoglycosides, carbapenems, piperacillin or piperacillin/tazobactam.
Multiresistant 3: intermediate or resistant to an agent in three of the following six categories: cephalosporins 2, fluoroquinolones 2, aminoglycosides, carbapenems, piperacillin or piperacillin/tazobactam, ampicillin/sulbactam.
Figure 8 – Percentage of Antibiotic Resistance in Certain Gram-Positive Bacteria, Certain Gram-Negative Bacteria and Pseudomonas sp., Québec, 2013-2014 (%)
Results per Healthcare Facility
Figures 9 and 10 show the breakdown of patient-periods monitored in 2013-2014, by type of vascular access and by healthcare facility. In 2013-2014, the percentage of fistulas decreased in 15 healthcare facilities and increased in 6 (Table 6). Twelve facilities reported a rate of 0 VARBSI per 100 patient-periods, and only one reported a rate higher than the 90th-percentile mark for 2009-2013 (Figure 11 and Table 7). Facilities with an incidence rate of 0 had small dialysis units of 4 to 12 chairs.
Figure 9 – Breakdown of Patient-periods Monitored by Type of Vascular Access and by Healthcare Facility, Québec, 2013-2014 (N)
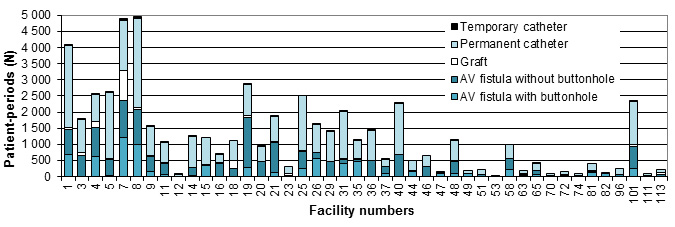
Figure 10 – Percentage of Patient-periods Involving a Fistula, by Healthcare Facility, Québec, 2013-2014 (%)
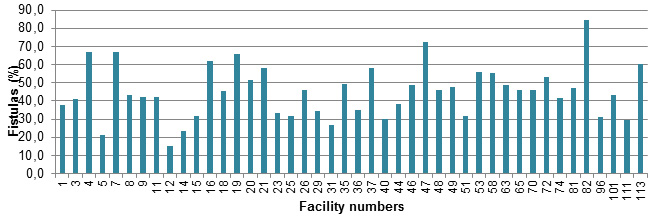
Figure 11 – VARBSI Incidence Rate per Healthcare Facility (2013-2014) and Incidence Rate Percentile (2009-2010 to 2012-2013), Québec, 2013-2014 (Incidence Rate per 100 Patient-periods)
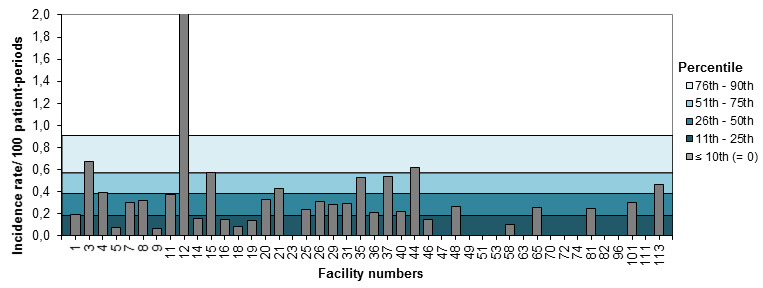
Table 6 – Number of Patient-periods Monitored and Percentage of Fistulas, by Healthcare Facility, Québec, 2009-2013 and 2013-2014 (N, % [95% CI])
| Facility | 2009-2013 | 2013-2014 | Variations | |||
|---|---|---|---|---|---|---|
Patients-periods (n) | % with fistula | Patients-periods (n) | % with fistula | |||
| 1 | HÔPITAL CHARLES LEMOYNE | 15,278 | 53 [52 ; 54] | 4,061 | 38 [36 ; 39] | diminution |
| 3 | HÔPITAL ROYAL VICTORIA | 7,570 | 43 [41 ; 44] | 1,789 | 41 [39 ; 44] |
|
| 4 | HÔPITAL NOTRE-DAME DU CHUM | 8,522 | 62 [61 ; 63] | 2,553 | 67 [65 ; 69] | augmentation |
| 5 | HÔPITAL GÉNÉRAL JUIF | 4,808 | 28 [26 ; 29] | 2,614 | 21 [20 ; 23] | diminution |
| 7 | PAVILLON L'HÔTEL-DIEU DE QUÉBEC | 14,241 | 51 [50 ; 51] | 4,897 | 67 [66 ; 68] | augmentation |
| 8 | PAV. MAISONNEUVE/PAV. MARCEL-LAMOUREUX | 18,927 | 50 [49 ; 51] | 4,954 | 43 [42 ; 45] | diminution |
| 9 | HÔPITAL DU HAUT-RICHELIEU | 5,046 | 44 [43 ; 46] | 1,554 | 42 [40 ; 45] |
|
| 11 | HÔPITAL PIERRE-LE GARDEUR | 4,148 | 45 [43 ; 46] | 1,055 | 42 [39 ; 45] |
|
| 12 | CENTRE HOSPITALIER UNIVERSITAIRE SAINTE-JUSTINE | 160 | 24 [18 ; 31] | 80 | 15 [7 ; 23] |
|
| 14 | CENTRE HOSPITALIER RÉGIONAL DE LANAUDIÈRE | 4,544 | 27 [26 ; 28] | 1,235 | 23 [21 ; 26] | diminution |
| 15 | HÔPITAL FLEURIMONT | 6,315 | 34 [32 ; 35] | 1,222 | 32 [29 ; 34] |
|
| 16 | HÔPITAL RÉGIONAL DE RIMOUSKI | 1,985 | 59 [57 ; 61] | 687 | 62 [58 ; 65] |
|
| 18 | HÔTEL-DIEU DE LÉVIS | 3,768 | 47 [45 ; 48] | 1,123 | 46 [43 ; 49] |
|
| 19 | HÔPITAL CITÉ DE LA SANTÉ | 5,647 | 68 [67 ; 69] | 2,869 | 66 [64 ; 68] | diminution |
| 20 | HÔPITAL DE CHICOUTIMI | 4,005 | 65 [63 ; 66] | 922 | 51 [48 ; 55] | diminution |
| 21 | HÔPITAL SAINT-LUC DU CHUM | 7,281 | 62 [60 ; 63] | 1,868 | 58 [56 ; 60] | diminution |
| 23 | HÔTEL-DIEU D'ARTHABASKA | 1,487 | 39 [36 ; 41] | 296 | 33 [28 ; 39] |
|
| 25 | HÔPITAL DU SACRÉ-COEUR DE MONTRÉAL | 7,538 | 26 [25 ; 27] | 2,517 | 32 [30 ; 33] | augmentation |
| 26 | HÔPITAL DE VERDUN | 6,416 | 51 [50 ; 52] | 1,610 | 46 [44 ; 49] | diminution |
| 29 | HÔPITAL GÉNÉRAL DE MONTRÉAL | 6,558 | 29 [28 ; 30] | 1,390 | 35 [32 ; 37] | augmentation |
| 31 | PAVILLON SAINT-JOSEPH | 8,352 | 28 [27 ; 29] | 2,027 | 27 [25 ; 29] |
|
| 35 | HÔPITAL HONORÉ-MERCIER | 1,889 | 53 [50 ; 55] | 1,125 | 49 [47 ; 52] |
|
| 36 | HÔPITAL GÉNÉRAL DU LAKESHORE | 3,314 | 40 [38 ; 42] | 1,428 | 35 [33 ; 38] | diminution |
| 37 | HÔTEL-DIEU DE SOREL | 2,499 | 52 [50 ; 54] | 560 | 58 [54 ; 62] | augmentation |
| 40 | HÔPITAL DE HULL | 9,297 | 33 [32 ; 34] | 2,281 | 30 [28 ; 32] | diminution |
| 44 | HÔPITAL SAINTE-CROIX | 2,038 | 42 [40 ; 44] | 483 | 38 [34 ; 43] |
|
| 46 | HÔPITAL DE GRANBY | 1,477 | 60 [58 ; 63] | 665 | 49 [45 ; 53] | diminution |
| 47 | HÔPITAL DE ROUYN-NORANDA | 854 | 64 [61 ; 68] | 138 | 72 [65 ; 80] |
|
| 48 | CENTRE HOSPITALIER DE ST. MARY | 2,973 | 44 [42 ; 46] | 1,113 | 46 [43 ; 49] |
|
| 49 | CSSS MEMPHRÉMAGOG | 374 | 48 [43 ; 53] | 192 | 47 [40 ; 54] |
|
| 51 | HÔPITAL DE MANIWAKI | 394 | 39 [34 ; 44] | 230 | 32 [26 ; 38] |
|
| 53 | HÔPITAL DE CHANDLER | - | - | 25 | 56 [37 ; 75] |
|
| 58 | HÔPITAL DU SUROÎT | 4,012 | 59 [57 ; 60] | 1,009 | 55 [52 ; 58] | diminution |
| 63 | HÔPITAL DE SAINT-GEORGES | 245 | 53 [46 ; 59] | 199 | 49 [42 ; 56] |
|
| 65 | HÔPITAL ET CLSC DE VAL-D'OR | 810 | 54 [51 ; 58] | 394 | 46 [41 ; 51] | diminution |
| 70 | CENTRE DE SOINS DE COURTE DURÉE LA SARRE | 240 | 67 [61 ; 73] | 94 | 46 [36 ; 56] | diminution |
| 72 | HÔPITAL ET CENTRE D'HÉBERGEMENT DE SEPT-ÎLES | 138 | 48 [39 ; 56] | 143 | 53 [45 ; 61] |
|
| 74 | HÔPITAL DE DOLBEAU-MISTASSINI | - | - | 96 | 42 [32 ; 52] |
|
| 81 | HÔPITAL DE MONT-LAURIER | 1,448 | 48 [45 ; 50] | 409 | 47 [42 ; 52] |
|
| 82 | PAVILLON SAINTE-FAMILLE | 234 | 60 [54 ; 66] | 102 | 84 [77 ; 91] | augmentation |
| 96 | CENTRE DE SANTÉ DE CHIBOUGAMAU | 490 | 40 [35 ; 44] | 239 | 31 [25 ; 37] | diminution |
| 101 | HÔPITAL RÉGIONAL DE SAINT-JÉRÔME | 9,048 | 45 [44 ; 46] | 2,322 | 43 [41 ; 45] |
|
| 111 | HÔPITAL DE PAPINEAU | - | - | 95 | 29 [20 ; 39] |
|
| 113 | HÔPITAL DE THETFORD MINES | 329 | 58 [53 ; 64] | 213 | 60 [54 ; 67] |
|
Table 7 – Number of VARBSI Cases and Incidence Rate by Healthcare Facility, and Percentile Ranking, Québec, 2009-2013 and 2013-2014 (Incidence Rate per 100 Patient-periods [95% CI])
| Facility | 2009-2013* | 2013-2014 | ||||
|---|---|---|---|---|---|---|
Number of cases | Mean Number of cases per year | Rate/100 pp | Number of cases | Rate/100 pp | ||
| 1 | HÔPITAL CHARLES LEMOYNE | 41 | 10.3 | 0.27 [0.19 ; 0.36] | 8 | 0.20 [0.08 ; 0.36] |
| 3 | HÔPITAL ROYAL VICTORIA | 49 | 12.3 | 0.65 [0.48 ; 0.84] | 12 | 0.67 [0.34 ; 1.10] |
| 4 | HÔPITAL NOTRE-DAME DU CHUM | 33 | 8.3 | 0.39 [0.27 ; 0.53] | 10 | 0.39 [0.19 ; 0.67] |
| 5 | HÔPITAL GÉNÉRAL JUIF | 12 | 6.0 | 0.25 [0.13 ; 0.41] | 2 | 0.08 [0.01 ; 0.22] |
| 7 | PAVILLON L'HÔTEL-DIEU DE QUÉBEC | 59 | 14.8 | 0.41 [0.32 ; 0.53] | 15 | 0.31 [0.17 ; 0.48] |
| 8 | PAV. MAISONNEUVE/PAV. MARCEL-LAMOUREUX | 85 | 21.3 | 0.45 [0.36 ; 0.55] | 16 | 0.32 [0.18 ; 0.50] |
| 9 | HÔPITAL DU HAUT-RICHELIEU | 45 | 11.3 | 0.89 [0.65 ; 1.17] | 1 | 0.06 [0.00 ; 0.25] |
| 11 | HÔPITAL PIERRE-LE GARDEUR | 26 | 6.5 | 0.63 [0.41 ; 0.89] | 4 | 0.38 [0.10 ; 0.84] |
| 12 | CENTRE HOSPITALIER UNIVERSITAIRE SAINTE-JUSTINE | 5 | 1.7 | 3.13 [0.99 ; 6.46] | 7 | 8.75 [3.47 ; 16.43] |
| 14 | CENTRE HOSPITALIER RÉGIONAL DE LANAUDIÈRE | 24 | 6.0 | 0.53 [0.34 ; 0.76] | 2 | 0.16 [0.02 ; 0.46] |
| 15 | HÔPITAL FLEURIMONT | 34 | 8.5 | 0.54 [0.37 ; 0.73] | 7 | 0.57 [0.23 ; 1.08] |
| 16 | HÔPITAL RÉGIONAL DE RIMOUSKI | 6 | 1.5 | 0.30 [0.11 ; 0.59] | 1 | 0.15 [0.00 ; 0.57] |
| 18 | HÔTEL-DIEU DE LÉVIS | 13 | 3.3 | 0.35 [0.18 ; 0.56] | 1 | 0.09 [0.00 ; 0.35] |
| 19 | HÔPITAL CITÉ DE LA SANTÉ | 16 | 8.0 | 0.28 [0.16 ; 0.44] | 4 | 0.14 [0.04 ; 0.31] |
| 20 | HÔPITAL DE CHICOUTIMI | 16 | 4.0 | 0.40 [0.23 ; 0.62] | 3 | 0.33 [0.06 ; 0.80] |
| 21 | HÔPITAL SAINT-LUC DU CHUM | 48 | 12.0 | 0.66 [0.49 ; 0.86] | 8 | 0.43 [0.18 ; 0.78] |
| 23 | HÔTEL-DIEU D'ARTHABASKA | 5 | 1.3 | 0.34 [0.11 ; 0.70] | 0 | 0.00 |
| 25 | HÔPITAL DU SACRÉ-COEUR DE MONTRÉAL | 43 | 10.8 | 0.57 [0.41 ; 0.75] | 6 | 0.24 [0.09 ; 0.47] |
| 26 | HÔPITAL DE VERDUN | 24 | 6.0 | 0.37 [0.24 ; 0.54] | 5 | 0.31 [0.10 ; 0.64] |
| 29 | HÔPITAL GÉNÉRAL DE MONTRÉAL | 35 | 8.8 | 0.53 [0.37 ; 0.73] | 4 | 0.29 [0.07 ; 0.64] |
| 31 | PAVILLON SAINT-JOSEPH | 25 | 6.3 | 0.30 [0.19 ; 0.43] | 6 | 0.30 [0.11 ; 0.58] |
| 35 | HÔPITAL HONORÉ-MERCIER | 10 | 5.0 | 0.53 [0.25 ; 0.91] | 6 | 0.53 [0.19 ; 1.05] |
| 36 | HÔPITAL GÉNÉRAL DU LAKESHORE | 6 | 2.0 | 0.18 [0.07 ; 0.35] | 3 | 0.21 [0.04 ; 0.52] |
| 37 | HÔTEL-DIEU DE SOREL | 19 | 4.8 | 0.76 [0.46 ; 1.14] | 3 | 0.54 [0.10 ; 1.31] |
| 40 | HÔPITAL DE HULL | 40 | 10.0 | 0.43 [0.31 ; 0.57] | 5 | 0.22 [0.07 ; 0.45] |
| 44 | HÔPITAL SAINTE-CROIX | 6 | 1.5 | 0.29 [0.11 ; 0.58] | 3 | 0.62 [0.12 ; 1.52] |
| 46 | HÔPITAL DE GRANBY | 4 | 1.3 | 0.27 [0.07 ; 0.60] | 1 | 0.15 [0.00 ; 0.59] |
| 47 | HÔPITAL DE ROUYN-NORANDA | 3 | 0.8 | 0.35 [0.07 ; 0.86] | 0 | 0.00 |
| 48 | CENTRE HOSPITALIER DE ST. MARY | 6 | 2.0 | 0.20 [0.07 ; 0.40] | 3 | 0.27 [0.05 ; 0.66] |
| 49 | CSSS MEMPHRÉMAGOG | 1 | 0.5 | 0.27 [0.00 ; 1.05] | 0 | 0.00 |
| 51 | HÔPITAL DE MANIWAKI | 3 | 1.5 | 0.76 [0.14 ; 1.87] | 0 | 0.00 |
| 53 | HÔPITAL DE CHANDLER | - | - | - | 0 | 0.00 |
| 58 | HÔPITAL DU SUROÎT | 10 | 2.5 | 0.25 [0.12 ; 0.43] | 1 | 0.10 [0.00 ; 0.39] |
| 63 | HÔPITAL DE SAINT-GEORGES | 1 | 0.5 | 0.41 [0.00 ; 1.60] | 0 | 0.00 |
| 65 | HÔPITAL ET CLSC DE VAL-D'OR | 4 | 2.0 | 0.49 [0.13 ; 1.10] | 1 | 0.25 [0.00 ; 1.00] |
| 70 | CENTRE DE SOINS DE COURTE DURÉE LA SARRE | 0 | 0.0 | 0.00 | 0 | 0.00 |
| 72 | HÔPITAL ET CENTRE D'HÉBERGEMENT DE SEPT-ÎLES | 1 | 0.5 | 0.72 [0.00 ; 2.84] | 0 | 0.00 |
| 74 | HÔPITAL DE DOLBEAU-MISTASSINI | - | - | - | 0 | 0.00 |
| 81 | HÔPITAL DE MONT-LAURIER | 1 | 0.3 | 0.07 [0.00 ; 0.27] | 1 | 0.24 [0.00 ; 0.96] |
| 82 | PAVILLON SAINTE-FAMILLE | 0 | 0.0 | 0.00 | 0 | 0.00 |
| 96 | CENTRE DE SANTÉ DE CHIBOUGAMAU | 0 | 0.0 | 0.00 | 0 | 0.00 |
| 101 | HÔPITAL RÉGIONAL DE SAINT-JÉRÔME | 62 | 15.5 | 0.69 [0.53 ; 0.87] | 7 | 0.30 [0.12 ; 0.57] |
| 111 | HÔPITAL DE PAPINEAU | - | - | - | 0 | 0.00 |
| 113 | HÔPITAL DE THETFORD MINES | 2 | 1.0 | 0.61 [0.06 ; 1.74] | 1 | 0.47 [0.00 ; 1.84] |
10th |
|
|
| 0.00 |
| 0.00 |
25th |
|
|
| 0.19 |
| 0.00 |
50th |
|
|
| 0.39 |
| 0.21 |
75th |
|
|
| 0.57 |
| 0.32 |
90th |
|
|
| 0.91 |
| 0.54 |
* Changes in rates within individual facilities were not subjected to statistical analysis, given the small number of cases involved
References
- Fistula First. Graphs of Prevalent AV Fistula Use Rates, By Network [online]. http://www.fistulafirst.org/AboutFistulaFirst/FisultaFirstCatheterLastFFCLData.aspx (last consulted: 2013-08-06).
- Ayzac, L., Machut, A., Russell, I., et al. Rapport final pour l’année 2011 du réseau de surveillance des infections en hémodialyse – DIALIN. CClin Sud-Est and RAISIN [online]. http://cclin-sudest.chu-lyon.fr/Reseaux/DIALIN/Resultats/rapport_annuel_2011_V2.pdf (last consulted: 2013-08-06).
- Patel, P. R., Yi, S. H., Booth, S., et al. Bloodstream Infection Rates in Outpatient Hemodialysis Facilities Participating in a Collaborative Prevention Effort: A Quality Improvement Report. American Journal of Kidney Diseases, Vol. 62, No. 2 (August 2013), p. 322–330.
Author
Comité de surveillance provinciale des infections nosocomiales (SPIN) – bactériémies associées aux accès vasculaires en hémodialyse
Editorial Committee
Élise Fortin, Direction des risques biologiques et de la santé au travail, Institut national de santé publique du Québec
Charles Frenette, Centre universitaire de santé McGill
Muleka Ngenda-Muadi, Direction des risques biologiques et de la santé au travail, Institut national de santé publique du Québec
Isabelle Rocher, Direction des risques biologiques et de la santé au travail, Institut national de santé publique du Québec
Mélissa Trudeau, Direction des risques biologiques et de la santé au travail, Institut national de santé publique du Québec